- Several studies have shown that facilitating access to EHC does NOT increase sexual or contraceptive risk-taking behaviour1
- A number of studies show that women and adolescents with greater access to EC are NOT more likely to engage in unprotected intercourse, and are more likely to adopt an ongoing contraceptive method after EHC use2,3
- Use of EHCs has NO effect on future fertility1,4
- If a woman is already pregnant, it is too late for EC. Emergency contraception does NOT interrupt an existing pregnancy or harm a developing embryo1,5
- EHCs do NOT protect against STIs.6 Only condoms protect against sexually transmitted infections.
- EHCs do NOT provide contraceptive cover for unprotected intercourse in the days following intake6
All posts by spin-inter

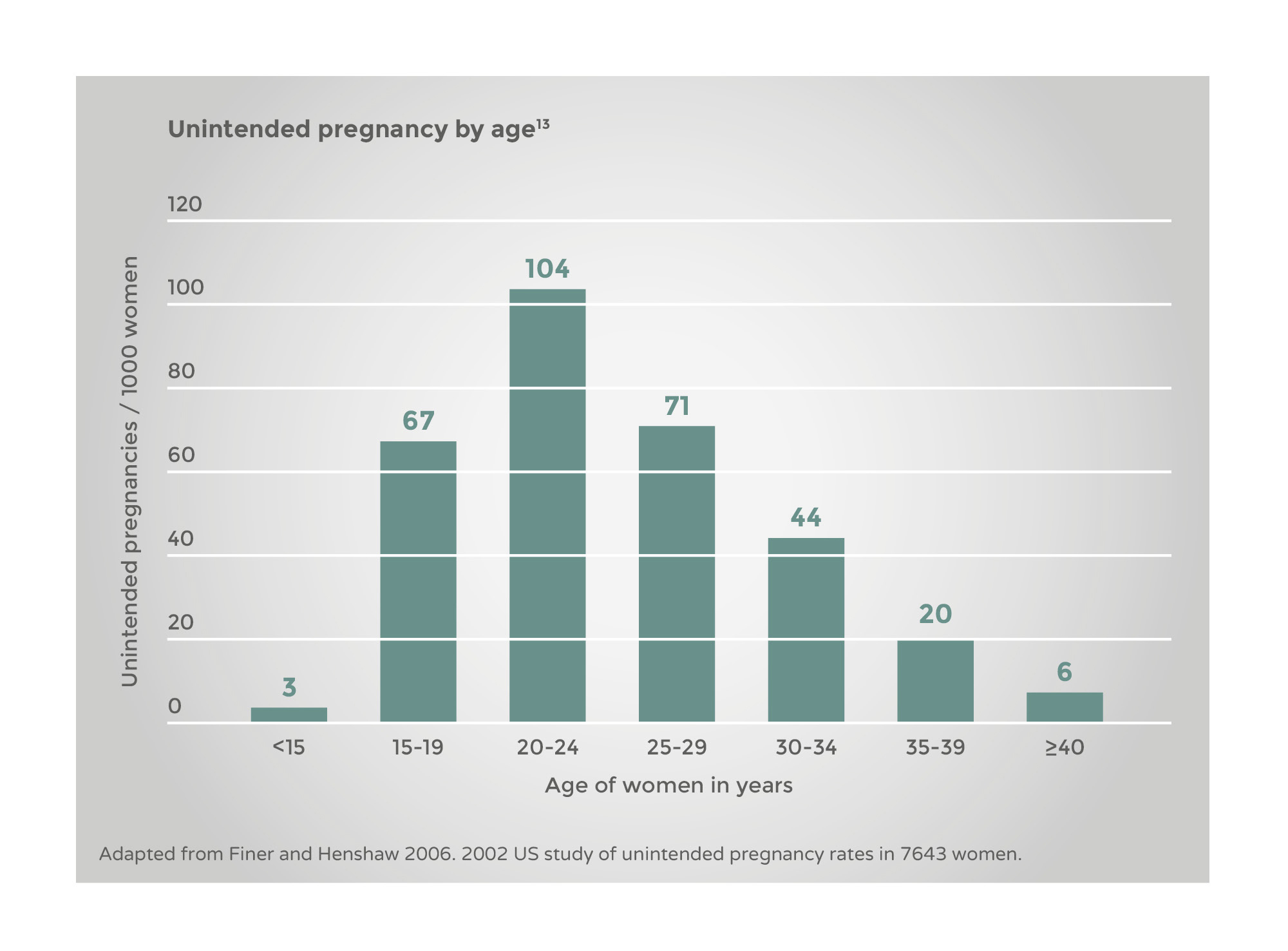
Unintended pregnancy happens at all reproductive ages, with a peak in women aged 20-24 years.1
During a woman’s mid-20s it is quite usual for relationships and contraception to be changing, although condoms are frequently used. These factors inevitably put women in this age bracket at risk of unintended pregnancy, despite responsible attitudes and sensible use of contraception.
As women get older, they may experience various lifestyle changes, such as being with a new partner, which may also put them at risk of unintended pregnancy.
It may be thought that the majority of women who request EHC do not use any contraceptive method.
However, research has shown that 67% of women who requested EHC are using a regular method of contraception (e.g. condom or pill)
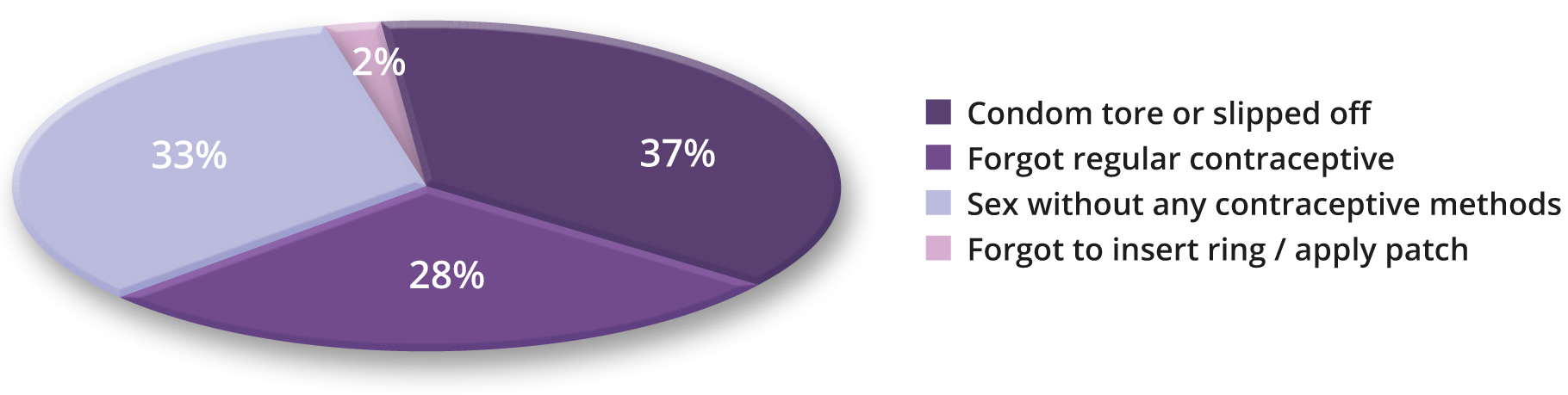
- Reasons for requesting emergency contraception
If we do the calculation, ‘contraceptive interruption’ is inevitable in a woman’s life, where she is trying to prevent pregnancy from the time she is about 17 years old (mean age of first sexual intercourse) until she is about 50. If she is on the Pill she will need to take about 8000 tablets correctly. It is unsurprising that she sometimes forgets tablets or makes mistakes.
It is important that women understand that ellaOne® is not a regular form of contraception.1 EC is not 100% effective and it is not as effective as a regular contraceptive method.
It is critical women understand that ellaOne® will not protect them from pregnancy if they have unprotected sex again after taking ellaOne®. They should use a reliable barrier contraceptive method until their next menstrual period, even if they are taking a regular contraceptive pill.2
EHC is not contraindicated to women using oral contraceptives but they should read the leaflet inside the pack to find out about continuing use of oral contraceptives in the month that they use ellaOne®.2 The package leaflet is also available online .
Fast access to ellaOne® after UPSI is important. When women come to your pharmacy seeking emergency contraception it is essential that your team know how to respond, so that women get the help they need to avoid unintended pregnancy.

Your team should know:
- Your pharmacy offers EHC
- Whether women requesting EHC must be referred to a pharmacist or if it can be dispensed by any team member
- Your aim is to offer women EHC in a reassuring way
In training sessions you could develop more examples or role-play the scenarios to build the team’s confidence so they can deal with requests for emergency contraception smoothly.
You can encourage your team to make the process of obtaining ellaOne® as least embarrassing as possible. They should recognise that this may be an emotional time for the woman. In a large EU survey, 50% of women said they found seeking EC embarrassing,1 so a welcoming, professional approach is appropriate. Other women may ask for EC in a way that may make you or your team members feel uncomfortable, maybe by providing too many intimate details or having a loud or brazen manner. Exploring ways to deal with this can also form part of a training role-play.
Sexuality and sexual behaviour are sensitive topics. They are part of our most private lives. When a woman asks for emergency contraception, she is disclosing that she had sexual intercourse and that the couple did not use, or had a problem with, their contraception.
When it comes to emergency contraception, some pharmacists can be confronted with his or her own prejudices. It is important to remember that couples and individuals have a right to decide freely and responsibly the timing and number of their children.1 Women who seek emergency contraception are behaving responsibly by taking steps to avoid unintended pregnancy. They need a warm approach. Treating all women in this way is always good practice, especially as some women may have been coerced to have sex (but not necessarily be disclosing this fact to you).
Unprotected sex or contraceptive failure can happen to anyone, for a number of different reasons.
Customers should always feel like they can talk to you openly and, in your role as a pharmacist, it is important to be able to have a professional conversation without judgement. There may be certain values and beliefs that you hold, but they must
never affect the advice you give. Always adhere to the General Pharmaceutical Council’s standards of conduct, ethics and performance. Principles such as “make patients your first concern” and “show respect to others” have particular relevance in the supply of ellaOne®.

| It can happen to anyone |
| Over a woman’s fertile life it would be most unusual if there were not occasional lapses in contraceptive cover |
| Love (and sex) are unpredictable, but dealing with unexpected events sensibly is the responsible thing to do |
| Women may stop their regular contraception for many reasons, including because they have no established partner |
| Human behaviour is complex and sometimes unpredictable |
| If she’s having sex she needs reliable contraception – including emergency contraception (provided within national guidelines where they exist) |
ellaOne® is contra-indicated for women who:
Are hypersensitive to the active substance or to any of the excipients1
Always refer to the ellaOne® Summary of Product Characteristics if you are in any doubt.
Situations where ellaOne® is not recommended
• Severe asthma treated by oral glucocorticoids1
• Severe hepatic impairment1
• For women taking CYP3A4 inducers1
• For women with long-term use of ritonavir1
• Concomitant use of EC containing levonorgestrel1
• Breastfeeding is not recommended for one week after ellaOne® intake1
With ellaOne®:
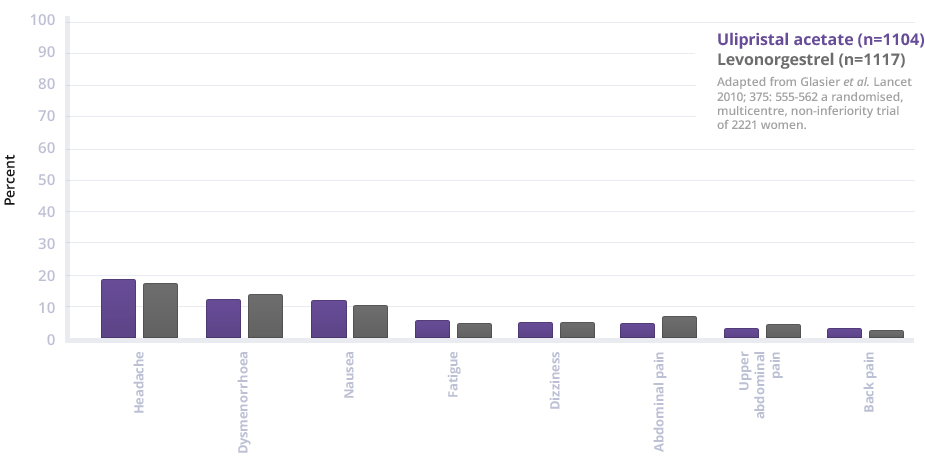
- The majority of adverse events recorded during the complete development programme in 4,718 women were mild or moderate and resolved spontaneously1
- The most commonly reported adverse reactions were headache, nausea, abdominal pain and dysmenorrhea1
- The tolerability profile is comparable to levonorgestrel2
ellaOne® effect on the menstrual cycle
Most women had their next menstrual period at the expected time (74.6 % within ±7 days of expected time)1
- Early period – 6.8% had their period more than 7 days earlier than expected
- Late period – 18.5% had a delay of more than 7 days1
A minority of women (8.7%) reported intermenstrual bleeding lasting an average of 2.4 days. The majority was reported as spotting (88.2%).1
Only 0.4% reported heavy intermenstrual bleeding1
For full details of adverse events refer to the ellaOne® Summary of Product Characteristics.
Adverse events should be reported. Healthcare professionals are asked to report any suspect adverse events via their national reporting system. Adverse events should also be reported to HRA Pharma at med.info.uk@hra-pharma.com
ellaOne® significantly reduces the risk of unintended pregnancy vs levonorgestrel.1
Two comparative non-inferiority studies showed ellaOne® is at least as effective in preventing pregnancy as levonorgestrel.1,2
A meta-analysis of these two studies comparing ellaOne® with levonorgestrel showed that the risk of pregnancy was significantly reduced with ulipristal acetate compared to levonorgestrel:1
For a woman who comes to you for help, what does this mean?


Her risk of getting pregnant is :
Intake within
of unprotected intercourse
- With
no intervention - With
levonorgestrel - With
ellaOne®
 5.5 %
5.5 %
5.5 % 2.3 %
2.3 %
2.2 % 0.9 %
0.9 %
1.4 %
P- value: 0.035
P- value: 0.046
Intake within 24 hours of unprotected intercourse / 72 hours of unprotected intercourse
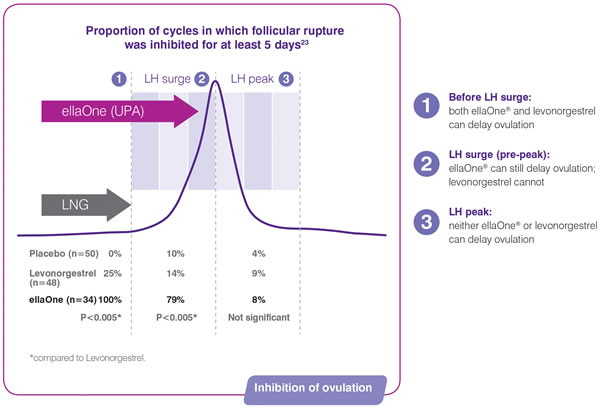
Ovulation is a result of a surge in luteinising hormone (LH). ellaOne® delays ovulation by inhibiting or delaying the LH surge.1
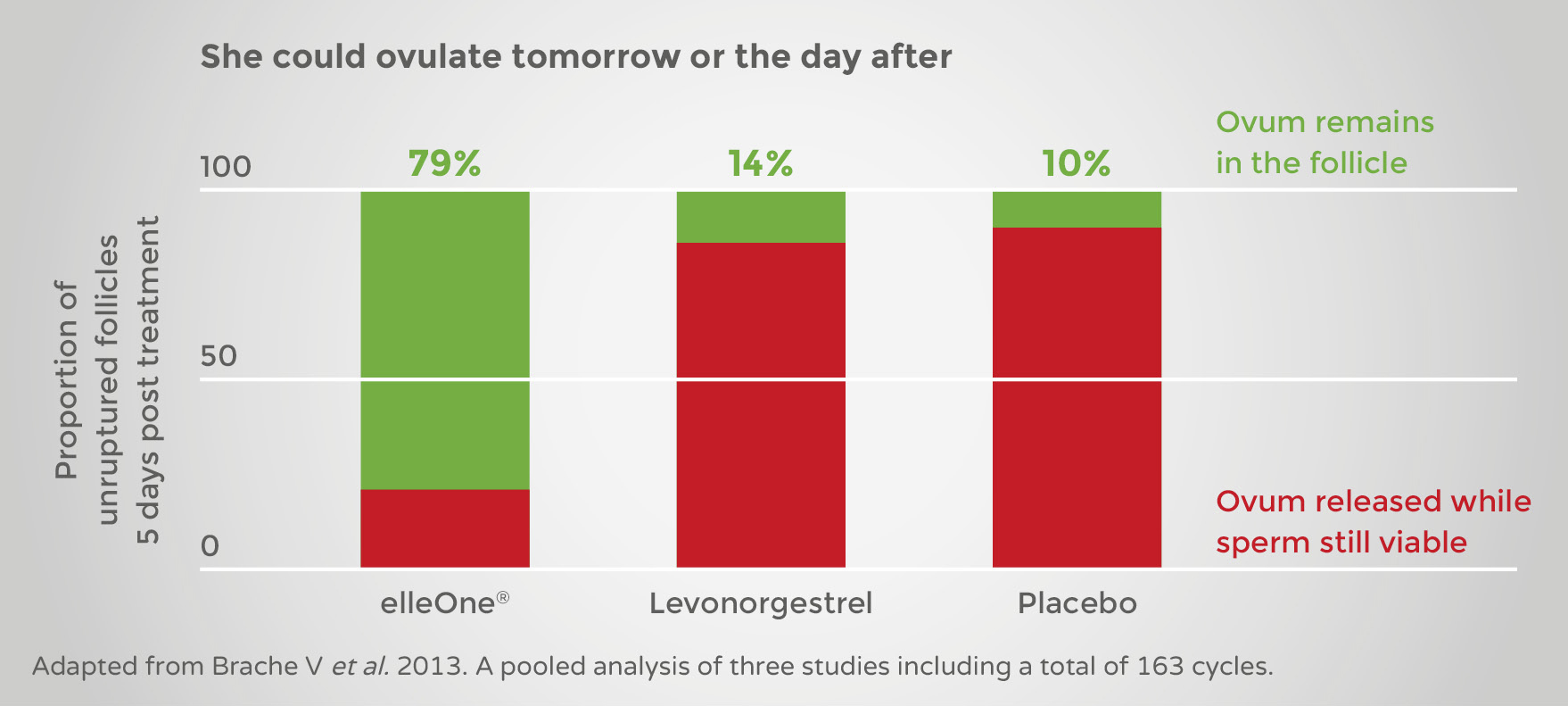
If the woman is due to ovulate tomorrow or the next day after unprotected sex, when the risk of pregnancy is highest, only ellaOne® can delay ovulation.1
This is when LH has started to surge but has not yet reached the peak. At this time, levonorgestrel will not prevent the follicle from rupturing whereas ellaOne® is highly effective.1
Intake after LH surge, but before peak1
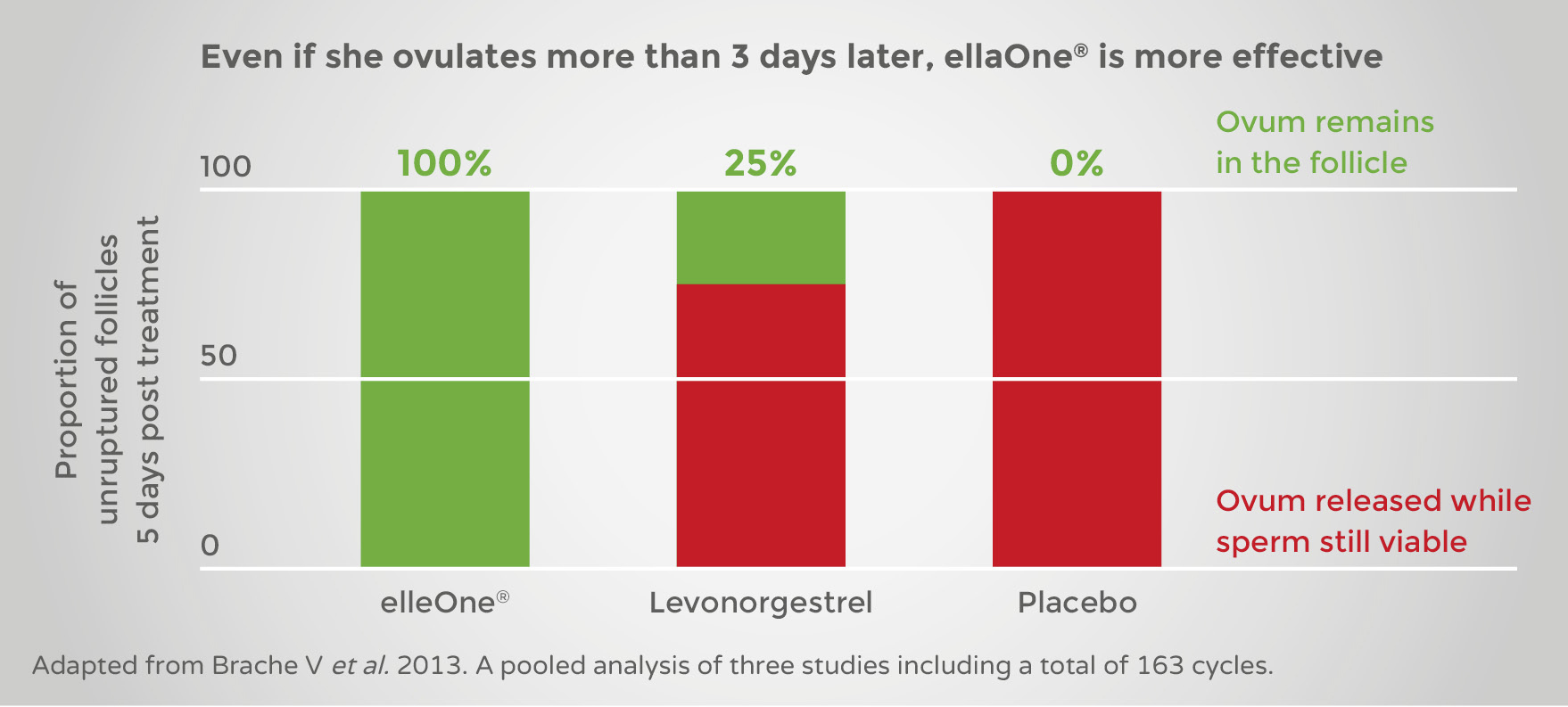
If she is due to ovulate 3 or more days after unprotected intercourse, both ellaOne and levonorgestrel can delay ovulation .1 However, ellaOne® remains more effective in preventing follicle rupture and therefore unintended pregnancy 1.
Intake before LH surge1
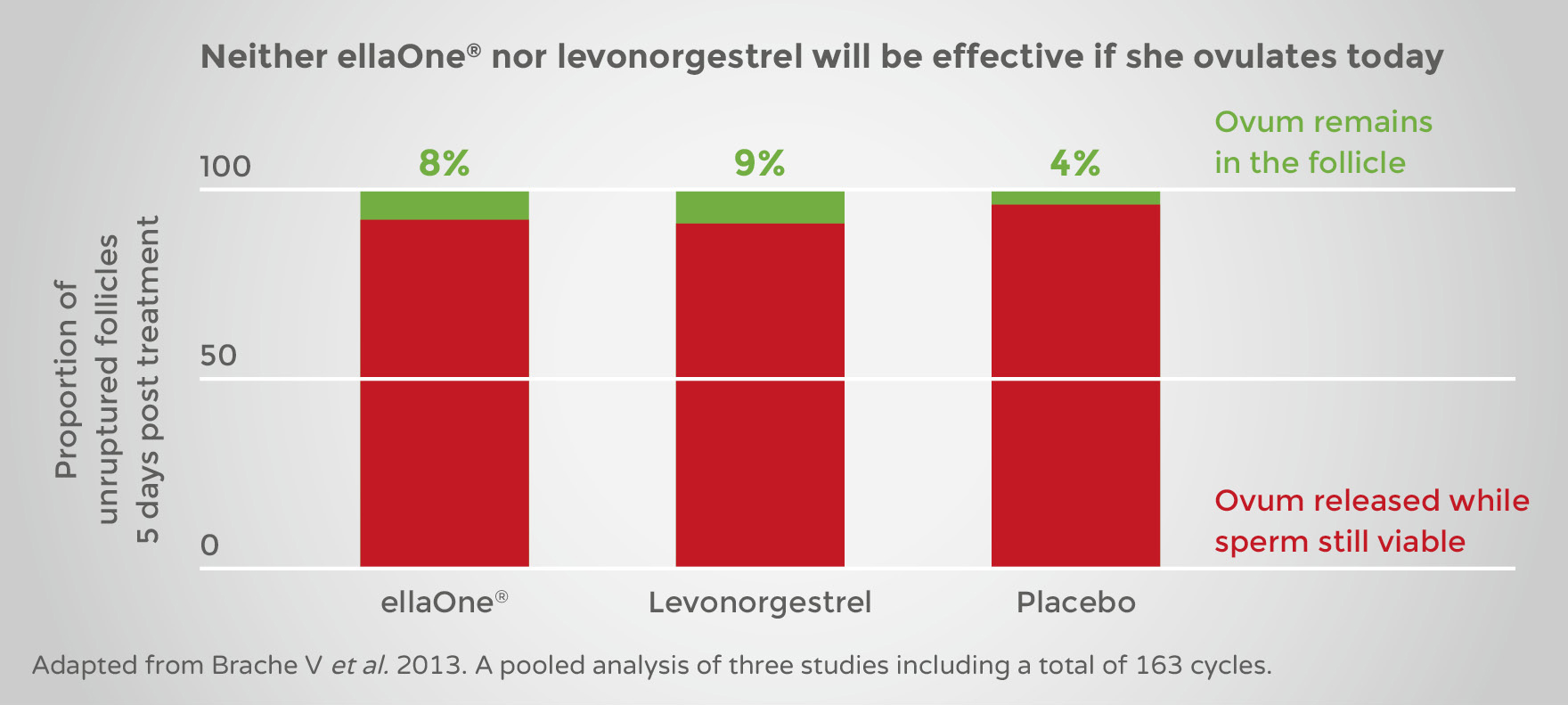
If the woman has already ovulated, or is due to ovulate, in the immediate 24 hours of unprotected intercourse, no emergency contraceptive pill help1
This is because the LH has already peaked, meaning the ovulation process is at a point where it cannot be stopped, or has already happened.
This explains why:
• Speed of emergency contraceptive pill intake is critical
• Emergency contraception is not 100% effective
Intake after LH surge 1
ellaOne® can delay ovulation even when it is about to happen (when risk of fertilisation is highest)1


